Colorectal Cancer—Clinician Recommendation Table
Who do these recommendations apply to?
These recommendations apply to asymptomatic adults aged 50 and older who are not at high risk for colorectal cancer (CRC). Adults are at high risk if they have at least one of the following:
- Previous CRC or adenomatous polyps (e.g., tubular or villous)
- Inflammatory bowel disease (e.g., ulcerative colitis or Crohn’s disease)
- Signs or symptoms of CRC (e.g., blood in the stool)
- History of CRC in one or more first-degree relatives
- Adults with hereditary syndromes predisposing to CRC (e.g., familial adenomatous polyposis or Lynch syndrome)
This tool provides guidance for primary care practitioners on different screening tests, screening intervals, and recommended ages to start and stop screening.
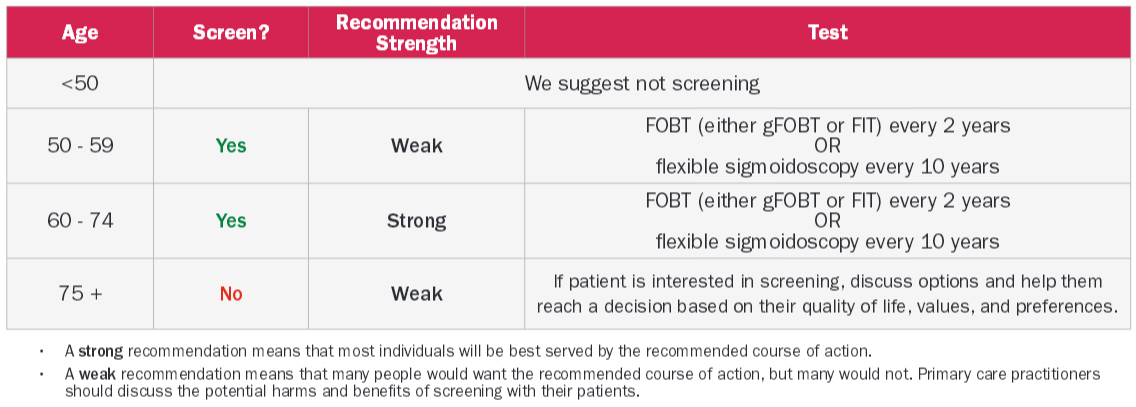
Resources, test availability, and patient preferences should be considered when choosing which screening test is appropriate.
Other recommendations
- We recommend not using colonoscopy as a primary screening test for CRC
- There is a lack of direct, high-quality evidence of the efficacy of colonoscopy in comparison to that of other screening tests.
- Colonoscopy has greater potential for harms (e.g., minor bleeding, major bleeding, perforation, and death) than the other available tests.
- Colonoscopy requires more time and expertise to perform, and using colonoscopy for screening means that this test will not be as readily available for people with symptomatic disease, such as visible blood in the stool.
Implementation considerations
- An FOBT test is the most convenient, uses the fewest resources, and will likely be the preferred option in most situations.
- It is important to note that flexible sigmoidoscopy is an option in specific circumstances based on patient values and preferences (e.g., averse to stool testing, prefers less frequent testing) and resource availability.
Evidence summary
- RCT data show that screening those aged 50-74 years for CRC with gFOBT or flexible sigmoidoscopy reduces the incidence of late-stage CRC and CRC mortality.
- FIT has greater sensitivity than gFOBT and similar specificity. Therefore, the reported mortality benefits of gFOBT for people aged 50-74 years can be extended to FIT.
- The only direct harms noted for either gFOBT or FIT in the studies reviewed were false positives and false negatives.
- The harms of flexible sigmoidoscopy are rare but include intestinal perforation, minor bleeding, major bleeding, and death